
A couple of years ago the London School of Tropical Medicine and Hygiene piloted its famous Diploma in Tropical Medicine course in East Africa. Obviously it’s been a huge success, as not only do you get to learn about exciting medicine from a world leading institute, you get to do it in vivo, with unequalled access to local expertise and clinical cases. As one of the many hopefuls applying for this course in 2013, I was interested to note human resources for health as their choice of topic for discussion on the enrolment form.
Human resource for health (HRH) involves analysing the distribution and quantity of healthcare workers worldwide, treating them in a similar way to more traditional ‘resources’ such as coal, minerals, etc. This allows for powerful analysis of the data available, which in turn is used by policy makers and governments to make decisions about the number of healthcare workers they need to train and employ.
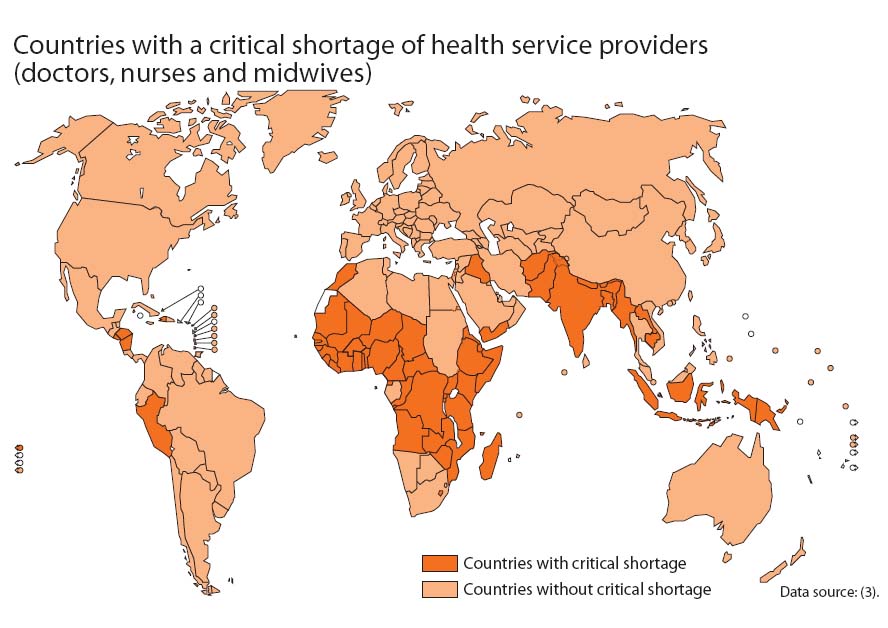
It is just such a topic where one might lead a wonderfully fulfilling life without being aware of its importance, until its implications are brought to bear on one’s health system. Almost universally, the statistics about HRH make for pretty grim reading. Did you know for instance that there is a worldwide shortage of health care professionals to the tune of about 4.3 million? Even worse, of the 57 countries deemed to have severe shortages of healthcare professionals, 36 are in Africa. One more shocking fact? Although Sub-Saharan Africa shoulders 24% of the world’s disease burden, it is home to only 3% of the world’s healthcare workers.
The reasons for this inequality include a lack of workers being trained, migration (the ‘brain drain’), anomalous data on HRH, and burden of disease. It’s a complex problem, and one that is gaining increasing recognition as being the next big barrier to improving healthcare in Africa. The development of the Millennium Development Goals has mobilised a lot of funding towards healthcare in Africa, but without the right people on the ground money alone cannot solve the problems.
We’ll be revisiting this topic on our trip, as well as reporting on any examples we encounter, and looking at the potential solutions to the HRH crisis.
(Image adapted from the WHO Health Report 2006)
